Project Overview
This project, developed in collaboration with Medtronic, addresses a critical issue in anterior cervical discectomy and fusion (ACDF) surgeries: post-operative dysphagia caused by bulky implant profiles.
The Challenge: Existing cervical plates provide necessary stabilization but often impinge on the pharynx wall due to excessive thickness and mass.
The Solution: We developed a “NextGen” low-profile plate system (1-level and 2-level) that maintains FDA-specified load-bearing capabilities while significantly reducing implant volume.
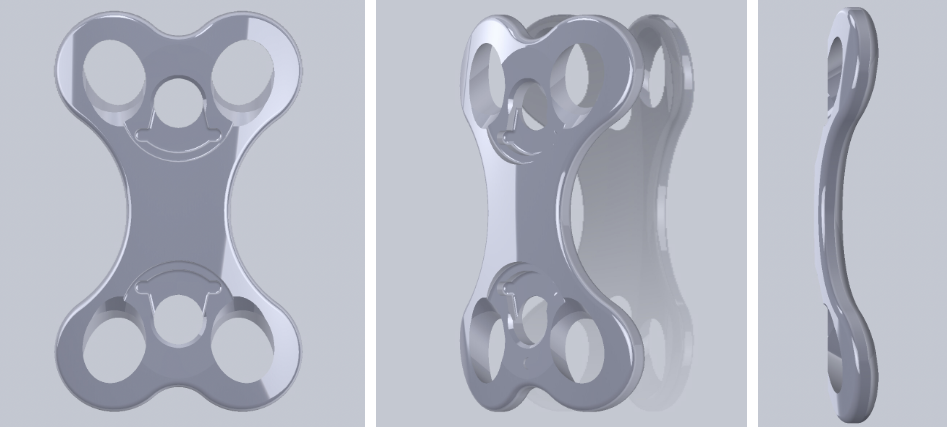

The Result: A topology-optimized implant that achieves a 20% reduction in mass and lower profile compared to the predicate device, validated through ASTM-F1717 computational testing.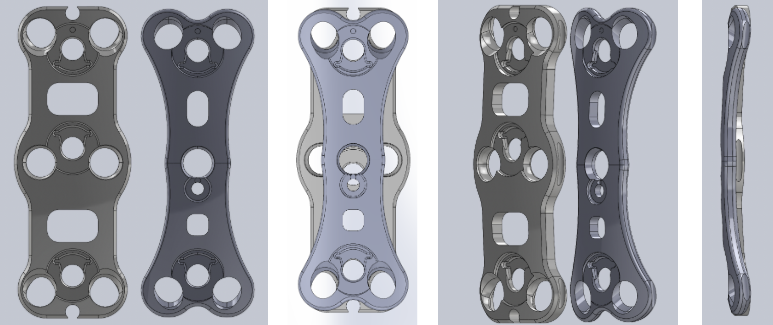
Mathematical Foundation
To reduce bulk without compromising safety, we utilized Topology Optimization.
1. Optimization Objective The goal was to minimize the mass ($M$) and compliance ($C$) of the plate to find the most efficient material layout:
$$\min_{x} \quad (1 - w) \frac{C(x)}{C_0} + w \frac{M(x)}{M_0}$$- $x$: Material density distribution variable.
- $w$: Weighting factor.
2. Constraints (Safety Factors) The optimization is constrained by the Von-Mises yield criterion to ensure the device never fails under physiological loads:
$$\sigma_{vm} \leq \frac{\sigma_{yield}}{SF}$$- Constraint: Minimize mass by 90% while maintaining global stress limits.
3. Load Cases (ASTM-F1717) We modeled the FDA-standard testing setup mathematically as a boundary value problem under three distinct loading conditions:
- Compression: Simulating head weight.
- Tension: Simulating neck extension.
- Torsion: Simulating neck rotation.
System Architecture (Design Process)
The development followed a rigorous V-Model engineering process:
- Requirements Definition: Mapped qualitative surgeon feedback (visibility, locking mechanism) to quantitative engineering specifications (profile thickness $< 2.0$mm, safety factor $> 1.5$).
- Topology Optimization: Used computational solvers to remove “dead mass” from non-load-bearing regions.
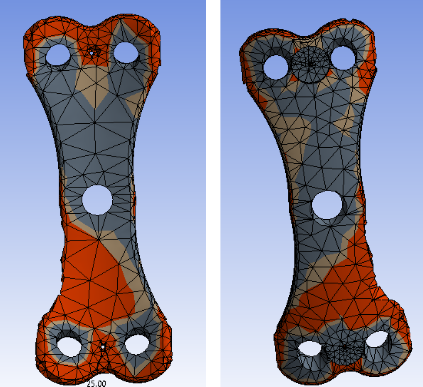
Figure 3: Topology Optimization - FEA Validation:
- Static Structural Analysis: Simulated the screw-plate interface and vertebral loads.
- Result: Final prototype showed peak stresses within safe limits (e.g., -28% displacement in compression vs predicate).
- Prototyping: 3D printed (SLA) and machined prototypes for fit-check validation with Medtronic surgical instrumentation.
Key Challenges & Resolutions
1. Geometric Constraints vs. Visibility
- Challenge: Surgeons require a clear “viewing window” to monitor bone graft fusion, but reducing material in the center weakens the plate.
- Resolution: We optimized the material layout specifically around the screw holes and locking mechanisms, creating a “truss-like” structure that preserved the central window while handling torsional loads.
2. Patent Landscape
- Challenge: The orthopedic device market is saturated with patents, making unique locking mechanisms difficult to design.
- Resolution: We adapted a standard “twist-lock” mechanism compatible with existing Medtronic drivers, ensuring the innovation focused on the plate topology rather than the commodity locking screw.
Future Work
- Fatigue Testing: Physical cyclic loading (10 million cycles) to validate long-term durability.
- Cadaver Labs: Surgical implantation trials to quantify the reduction in tissue retraction required.